The Science
Why inhaled delivery may offer a better approach to treating anaphylaxis
The Challenge
Anaphylaxis Progresses in Minutes
Anaphylaxis is a cascade reaction. Once triggered, mast cells and basophils rapidly release histamine and other mediators that drive the clinical symptoms: vasodilation, bronchoconstriction, mucosal edema.
Published research shows mediator release begins within 2 minutes of allergen exposure, with reaction severity correlating with early histamine and PAF levels.1,2 Mediator production continues for approximately 15 minutes before tapering, while symptoms typically begin within 10 minutes of exposure.3
This creates a narrow treatment window. Effective intervention requires two things:
Stabilize Mast Cells and Basophils
Prevent further degranulation and mediator release
Reverse Symptoms
Counteract the effects of mediators already released
Epinephrine is the only treatment that addresses both. It stabilizes mast cells and basophils via β2-adrenergic receptors while reversing symptoms through α1 and β2 receptor activation. The question is how to deliver it most effectively.
Recent research on inhaled epinephrine demonstrates rapid systemic availability, with peak plasma concentrations achieved in approximately 2 minutes via the pulmonary route.4 This pharmacokinetic profile has generated interest in inhaled delivery as an approach to anaphylaxis treatment.
The Target
Why the Lung
Mast cells concentrate at the body's interfaces with the external environment, with particularly high density in the airways.5 The lungs present by far the largest absorptive surface of any tissue exposed to the external environment.
Inhalation delivery can achieve substantially higher local drug concentrations in lung tissue compared to systemic delivery. For example, published data for another inhaled drug (aztreonam) show that a 75 mg inhaled dose achieved lung sputum concentrations approximately 200 times higher than a 2 g intravenous dose.11,12
Tissue Surface Area Comparison
| Tissue | Surface Area |
|---|---|
| Airways / Lungs | 70–130 m² |
| GI Tract | ~32 m² |
| Skin | ~2 m² |
Sources: Fröhlich et al. Front Pharmacol. 2016; Helander & Fändriks. Scand J Gastroenterol. 2014.
Postmortem studies of fatal anaphylaxis consistently show strong mast cell activation in lung tissue. In one systematic review, 100% of cases showed lung involvement.6,7
This distribution suggests the lung may be a primary target for mast cell stabilization. Whether this translates to clinical benefit for inhaled epinephrine delivery is being evaluated in clinical studies.
Clinical Insight
40 Years of Observation
Since 1993, Dr. George Luciuk, an allergist and former President of the Allergy Section of the Canadian Pediatric Society, has been working to develop improved treatments for patients experiencing allergic reactions with inhaled epinephrine via metered dose inhalers.
Across thousands of treatments and multiple types of inhaler, a pattern emerged:
Upper airway symptoms (laryngeal/pharyngeal edema) showed improved resolution. Systemic symptoms (hypotension, pruritis) had incomplete reversal.
Systemic symptoms (hypotension, pruritis) resolved effectively. Upper airway symptoms (laryngeal/pharyngeal edema) responded poorly and less completely.
Different products deposited drug differently, some favoring the throat, others the deep lung. These clinical outcomes were dependent on the aerosol drug delivery characteristics.
The distinction is critical. Prior conclusions about inhaled epinephrine were based on poor aerosol drug delivery. The question was not whether the lung was the right target, but whether a product could be designed to address both upper airway and systemic delivery. KP001 (REZQPUFF) was developed as a fit-for-purpose product to address this challenge.
Our Approach
Designing for Dual Delivery
Kokua Pharma partnered with a leading aerosol research institution to understand why different formulations showed different clinical effects.
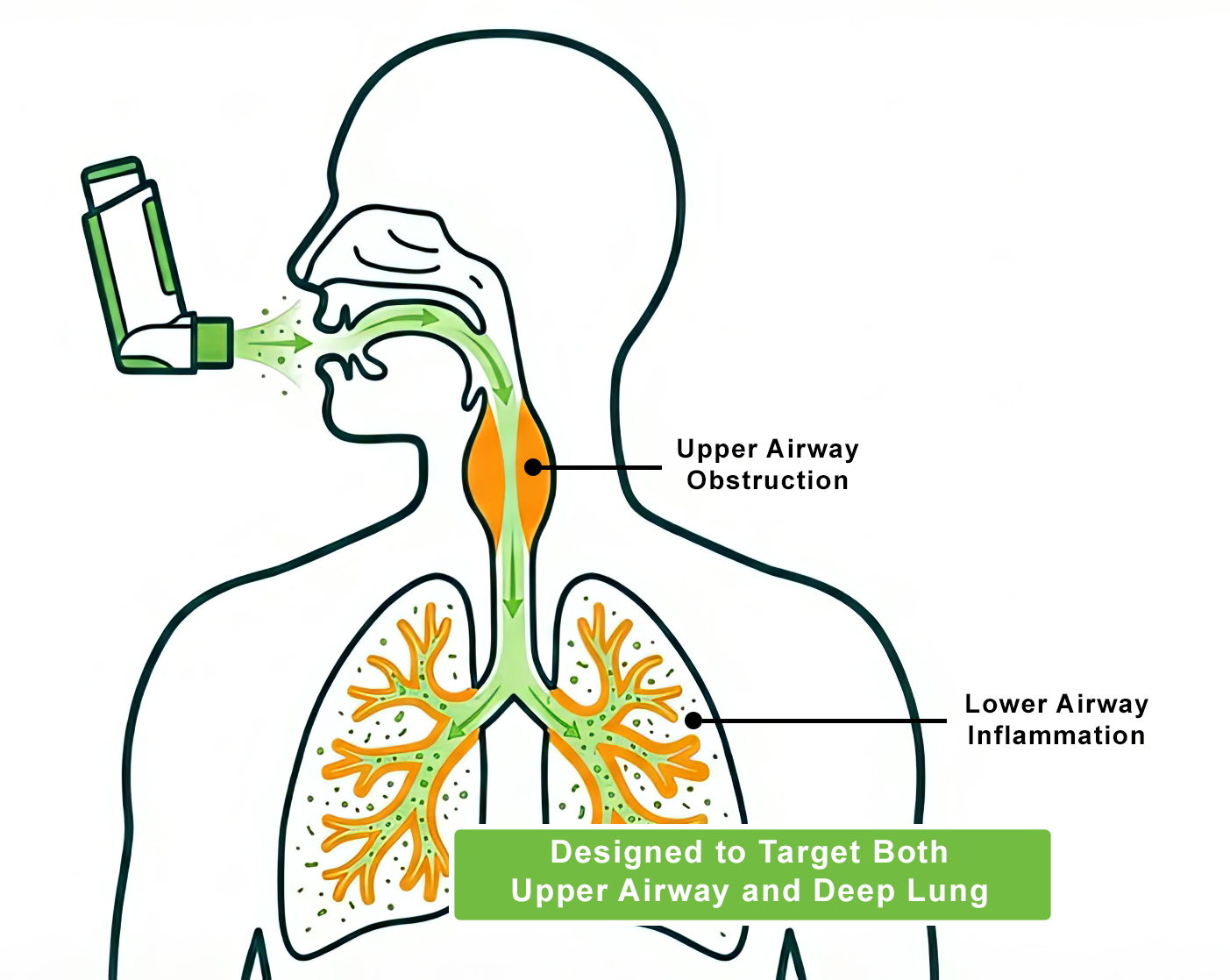
The answer lay in drug deposition patterns. By optimizing the aerosol delivery characteristics, it may be possible to achieve meaningful deposition in both:
Upper Airway
Local effect on laryngeal and pharyngeal edema
Deep Lung
Systemic absorption and mast cell stabilization
Inhaled (KP001)
Direct airway delivery and systemic absorption
Nasal Spray
Systemic via nasal mucosal absorption
IM Injection
Systemic via muscle injection
Illustrative comparison of delivery mechanisms. KP001 (REZQPUFF) is investigational and not yet FDA-approved.
Design Objectives
Targeted throat deposition for upper airway delivery
Deep lung delivery for systemic absorption and mast cell stabilization
Orientation-independent performance for real-world use
Consistent delivery across breathing patterns
Additional Benefit
Preservative-Free
Dr. Luciuk's clinical experience included treating sulfite-sensitive patients, who face a particular challenge: all currently approved epinephrine auto-injectors and nasal spray products for anaphylaxis self-treatment contain sodium metabisulfite as a preservative.
Published studies report that sulfite sensitivity affects an estimated 5-10% of chronic asthmatic patients.8
Published case reports document adverse reactions to sulfite preservatives in medications, including bronchospasm, anaphylaxis, and instances where sulfite-containing epinephrine treatments provoked worsening symptoms rather than relief.13,14,15,16
In a study presented at AAAAI 2026, 20 patients reporting cosmetic-related skin reactions underwent skin prick testing with serial dilutions of epinephrine injection containing metabisulfite. All 20 exhibited moderate-to-severe systemic allergic responses (WAO Grade 2-5), suggesting metabisulfite sensitivity may have a higher prevalence than currently recognized.10
KP001 (REZQPUFF) is being developed as a preservative-free formulation, which may be relevant for patients with sensitivity to sulfite preservatives found in existing epinephrine products.9
Scientific Publications
Published Research
The following studies have been published in peer-reviewed journals and presented at scientific conferences:
The Pharmacokinetics of a Novel Inhaled Epinephrine
Luciuk GH, Discepola L, Pimstone S, Stapleton KW. J Allergy Clin Immunol. 2026;157(2 Suppl):Abstract L80. AAAAI 2026.
View Poster →Time to Symptom Resolution: An Efficacy Endpoint for the Effectiveness of Anaphylaxis Treatments
Luciuk GH, Discepola L, Pimstone S, Stapleton KW. J Allergy Clin Immunol. 2026;157(2 Suppl):Abstract 597. AAAAI 2026.
View Poster →Implications of a Significant Cosmetic Allergy
Luciuk GH, Discepola L, Pimstone S, Stapleton KW. J Allergy Clin Immunol. 2026;157(2 Suppl):Abstract 596. AAAAI 2026.
View Poster →Development of a Metered Dose Inhaler for the Treatment of Anaphylaxis in Metabisulfite Sensitive Patients
Ruzycki CA, Schuster V, Tavernini S, Finlay WH, Martin AR, Stapleton KW, Luciuk G. Ann Allergy Asthma Immunol. 2025;135(5 Suppl 1):S16-S17.
View Poster → View Publication →Effect of pMDI Orifice Diameter on Regional Extrathoracic Deposition in an Idealized Child Airway
Pillay K, Tavernini S, Ruzycki CA, Luciuk G, Stapleton K, Finlay WH, Martin AR. Pharm Res. 2026. doi:10.1007/s11095-026-04048-w
View Poster → View Publication →References
- Halmerbauer G, et al. In vivo histamine release during the first minutes after deliberate sting challenges correlates with the severity of allergic symptoms. Pediatr Allergy Immunol. 1999;10:53-57. DOI
- Ma X, Xiaokaiti Y, Lei H, et al. Epinephrine inhibits vascular hyperpermeability during platelet-activating factor- or ovalbumin-induced anaphylaxis. RSC Adv. 2017;7(83):52762-52771. DOI
- van der Linden PWG, et al. Insect-sting challenge in 138 patients: relation between clinical severity of anaphylaxis and mast cell activation. J Allergy Clin Immunol. 1992;90(1):110-118. DOI
- Zhang JY, et al. Comparison of Systemic Exposure Between Epinephrine Delivered via Metered-Dose Inhalation and Intramuscular Injection. J Aerosol Med Pulm Drug Deliv. 2025;38(2):71-82. DOI
- Metcalfe DD, Baram D, Mekori YA. Mast cells. Physiol Rev. 1997;77(4):1033-1079. DOI Surface area data from Fröhlich E, et al. Front Pharmacol. 2016; Helander HF, Fändriks L. Scand J Gastroenterol. 2014.
- Esposito M, et al. Anaphylactic Death: A New Forensic Workflow for Diagnosis. Healthcare. 2021;9(2):117. PubMed
- Del Duca F, et al. Death Due to Anaphylactic Reaction: The Role of the Forensic Pathologist. Medicina (Kaunas). 2023;59(12). DOI
- Gunnison AF, Jacobsen DW. Sulfite Hypersensitivity. A Critical Review. CRC Critical Reviews in Toxicology. 1987;17(3):185-214. DOI
- Roth JV, Shields A. How does one treat anaphylaxis in the sulfite-allergic patient? Anesth Analg. 1999;88(1):222. DOI
- Luciuk GH, Discepola L, Pimstone S, Stapleton KW. Implications of a Significant Cosmetic Allergy. J Allergy Clin Immunol. 2026;157(2 Suppl):Abstract 596. AAAAI 2026. View Poster
- Bechard DL, Hawkins SS, Dhruv R, Friedhoff LT. Penetration of aztreonam into human bronchial secretions. Antimicrob Agents Chemother. 1985;27(2):263-264. DOI
- Gilead Sciences. Cayston (Aztreonam) Inhalation Solution Label. 2024. FDA/MedWatch. DailyMed
- Twarog FJ, Leung DY. Anaphylaxis to a component of isoetharine (sodium bisulfite). JAMA. 1982;248(16):2030-2031. JAMA
- Frick WE, Lemanske RF. Oral sulfite sensitivity and provocative challenge in a 2 year old. J Asthma. 1991;28(3):221-224. DOI
- Riggs BS, Harchelroad FP, Poole C. Allergic reaction to sulfiting agents. Ann Emerg Med. 1986;15(1):77-79. DOI
- Luciuk GH. Adrenalin Anaphylaxis. J Allergy Clin Immunol. 1993;91(1, Part 2):53. JACI
Business Development